This calculator is designed to assist radiologists and trainees in assessing thyroid nodule risk using the American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS). This thyroid ultrasound scoring system provides a structured framework for evaluating nodules and estimating malignancy risk, making it a valuable tool for clinical decision-making. By combining sonographic features into a cumulative score, the calculator supports evidence-based recommendations for biopsy or surveillance and streamlines thyroid nodule risk assessment in everyday practice.
The clinical management of thyroid nodules has evolved significantly with the widespread adoption of the American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS). Designed to address the high prevalence of incidental thyroid nodules detected in up to 68% of high-resolution ultrasound examinations and the associated potential for overdiagnosis, the TI-RADS calculator provides a standardized, quantitative framework for malignancy risk stratification.
Unlike European (EU-TIRADS) or Korean (K-TIRADS) systems which rely on pattern recognition, this thyroid ultrasound scoring tool utilizes a point-based methodology. This approach weights individual sonographic features based on their positive predictive value (PPV) for malignancy. By prioritizing high specificity, the thyroid nodule risk calculator aims to significantly reduce the volume of unnecessary fine-needle aspiration (FNA) biopsies of benign or indolent lesions while maintaining sensitivity for clinically significant disease.
This reference guide details the scoring mechanics, clinical interpretation, reporting nuances, and limitations essential for board-certified radiologists and trainees utilizing the TI-RADS calculator.
The Five Ultrasound Feature Categories
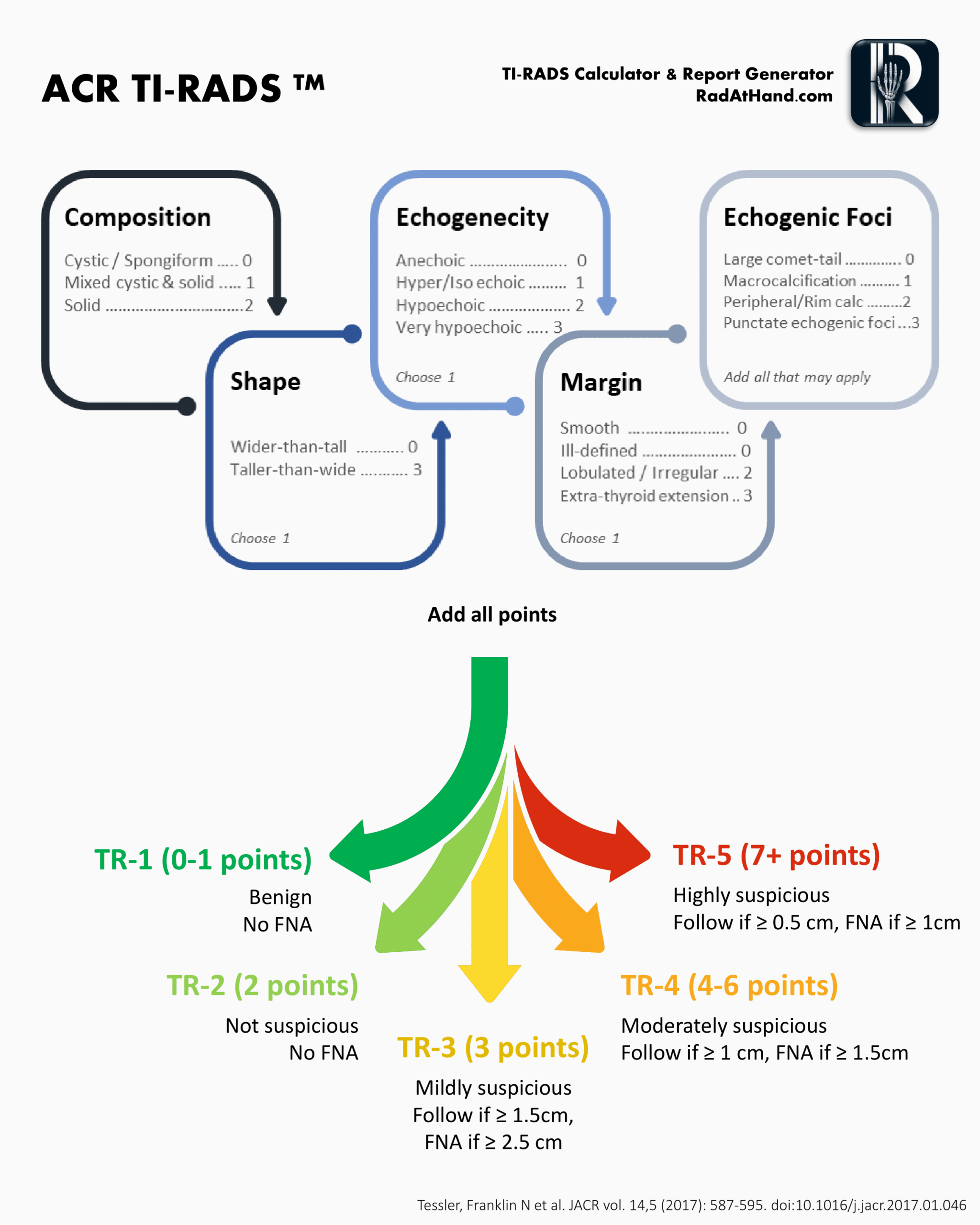
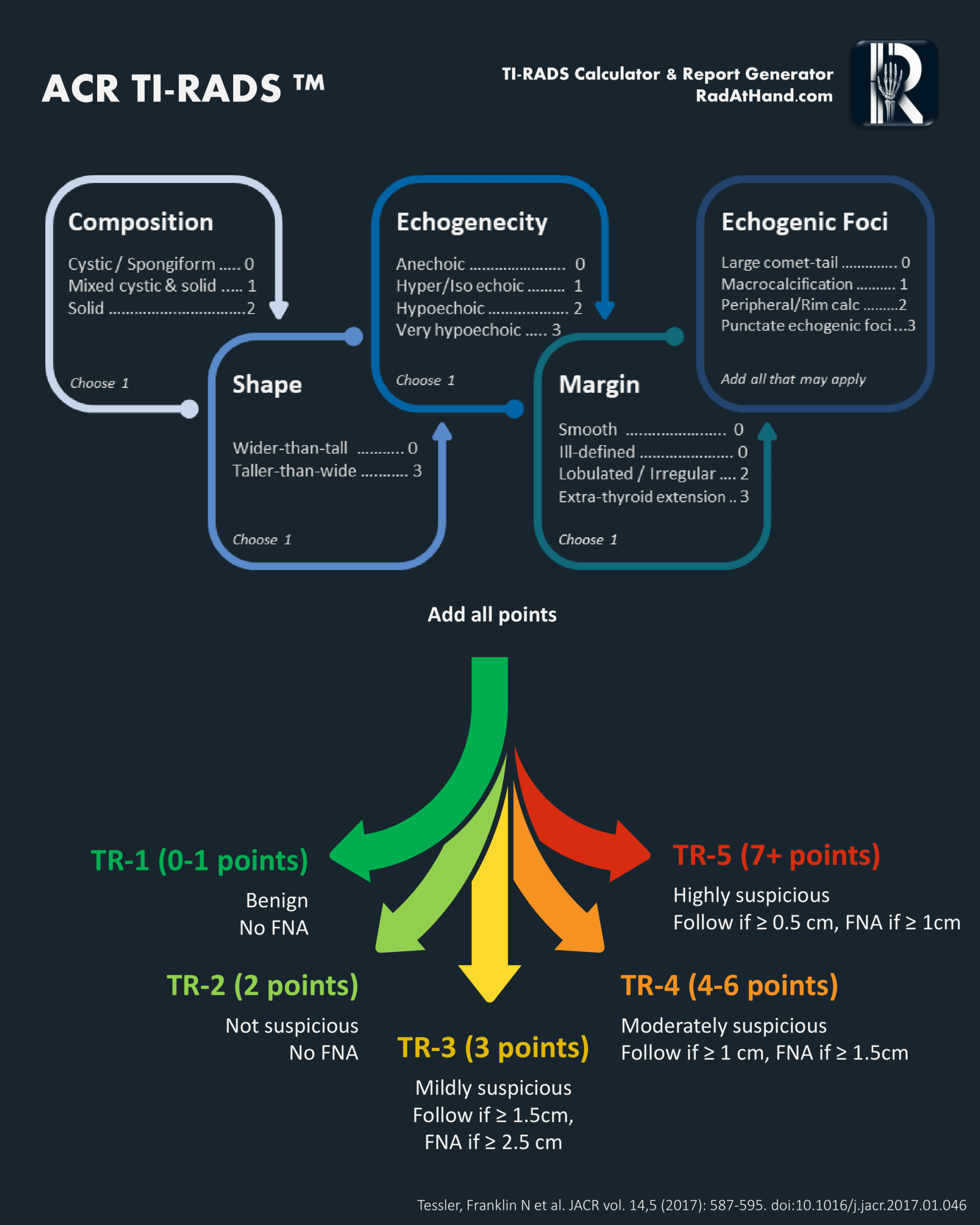
The TI-RADS risk assessment derives a cumulative score from five sonographic categories. Points are assigned based on the feature most suspicious for malignancy within each category. This weighted system ensures that high-risk features contribute disproportionately to the total score generated by the thyroid ultrasound scoring tool, accurately reflecting the increased probability of malignancy.
1. Composition
This category assesses the internal architecture of the nodule.
- Cystic or almost completely cystic (0 points): These lesions are benign and require no further scoring.
- Spongiform (0 points): Defined as composed of greater than 50% small cystic spaces, this appearance is highly specific for benignity.
- Mixed cystic and solid (1 point): This applies regardless of the proportion of the solid component, provided it does not meet spongiform criteria.
- Solid or almost completely solid (2 points): This feature carries a higher risk association. For scoring purposes, visual estimation of >95% solid is sufficient.
2. Echogenicity
Echogenicity is evaluated relative to the surrounding thyroid parenchyma and the anterior neck musculature. For mixed nodules, the score is based exclusively on the solid component.
- Anechoic (0 points): Applies to cystic fluid.
- Hyperechoic or Isoechoic (1 point): Increased or similar echogenicity relative to the thyroid parenchyma.
- Hypoechoic (2 points): Less echogenic than thyroid parenchyma.
- Very Hypoechoic (3 points): Less echogenic than the adjacent strap muscles. This is a specific indicator of malignancy and carries significant weight in the TI-RADS calculator.
3. Shape
Shape is assessed exclusively in the transverse (axial) plane.
- Wider-than-tall (0 points): The anteroposterior diameter is less than or equal to the transverse diameter (parallel orientation).
- Taller-than-wide (3 points): The anteroposterior diameter exceeds the transverse diameter (non-parallel orientation). This feature reflects centrifugal growth against tissue planes and is a strong independent predictor of malignancy.
4. Margin
This category evaluates the interface between the nodule and the surrounding tissue.
- Smooth (0 points): Uninterrupted, well-defined border.
- Ill-defined (0 points): The border merges imperceptibly with the thyroid parenchyma. It is critical to distinguish this from an infiltrative margin; ill-defined margins in isolation are generally benign.
- Lobulated or Irregular (2 points): Spiculated or jagged edges, or protrusions into the parenchyma.
- Extrathyroidal Extension (3 points): Frank invasion into adjacent soft tissue or vascular structures. Mere bulging of the capsule does not qualify as extension.
5. Echogenic Foci
Unlike other categories where a single feature is selected, multiple features can be selected in this category, and their points are additive.
- None or Large Comet-tail Artifacts (0 points): V-shaped artifacts >1 mm in depth are typically associated with colloid and benignity.
- Macrocalcifications (1 point): Coarse calcifications with posterior acoustic shadowing.
- Peripheral (Rim) Calcifications (2 points): Calcification along the nodule margin. These should be scrutinized carefully, as complete shadowing may obscure central malignant components.
- Punctate Echogenic Foci (3 points): These correspond to psammomatous calcifications associated with papillary thyroid carcinoma. They are smaller than macrocalcifications and lack the deep V-shaped tail of colloid artifacts.
Clinical Interpretation: TR Categories and Management with the TI-RADS Calculator
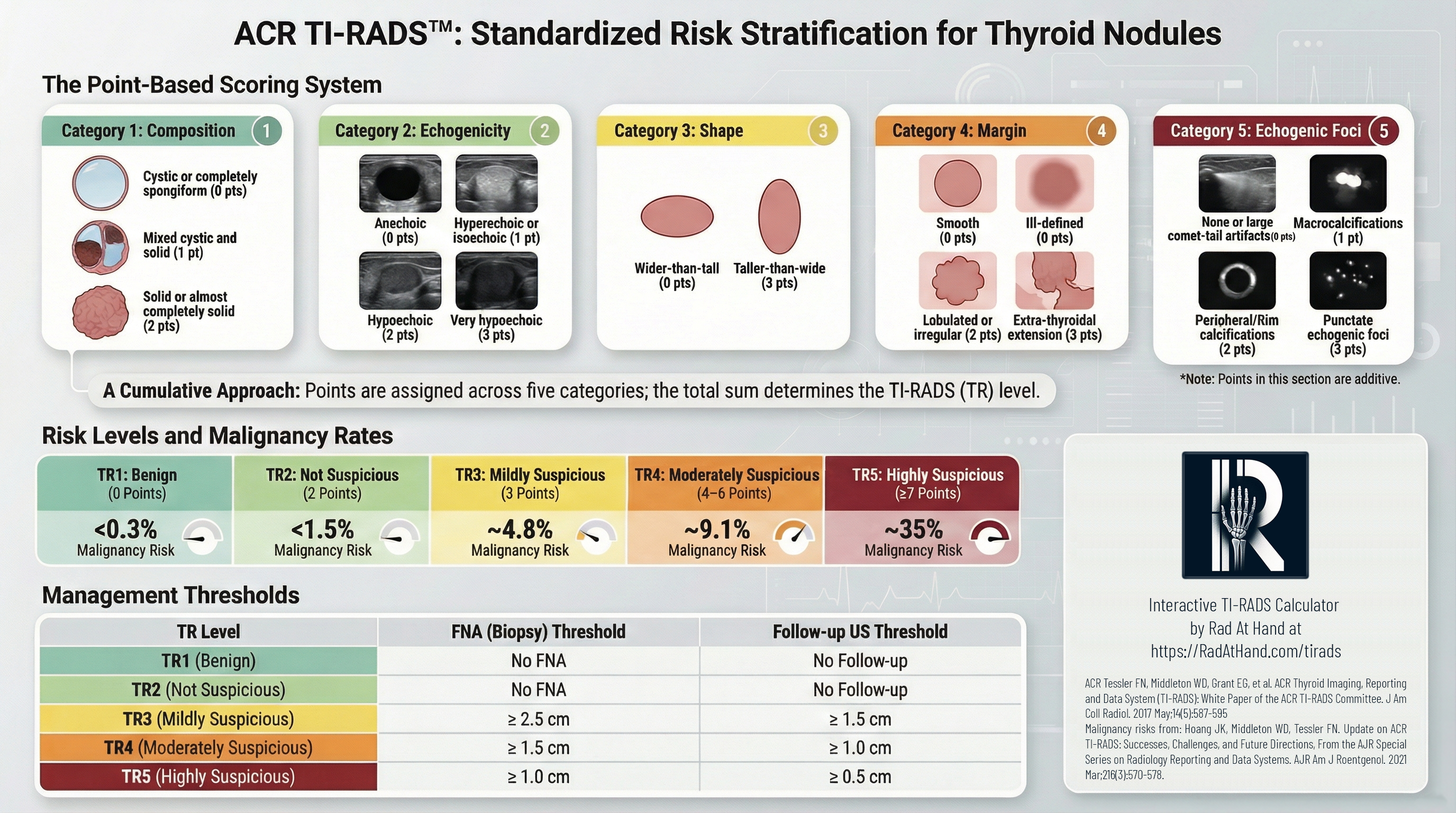
The sum of points determines the TI-RADS (TR) level. This TI-RADS risk assessment score correlates with malignancy risk and dictates size-based management thresholds.
A defining characteristic of the ACR TI-RADS is the intentional use of higher size thresholds for biopsy compared to other international guidelines. This shift is largely driven by the reclassification of Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features (NIFTP). Recognizing NIFTP as an indolent lesion, the ACR established these thresholds to minimize the overtreatment of non-threatening neoplasms, prioritizing clinical significance over mere detection.
Table: ACR TI-RADS TR categories and management recommendations using the TI-RADS calculator| Category | Points | Malignancy Risk | Management |
|---|
| TR1: Benign | 0 | < 0.3% | No FNA required. |
| TR2: Not Suspicious | 2 | ~1.5% | No FNA required. |
| TR3: Mildly Suspicious | 3 | ~4.8% | FNA if ≥ 2.5 cm
Follow-up US if ≥ 1.5 cm |
| TR4: Moderately Suspicious | 4-6 | ~9.1% | FNA if ≥ 1.5 cm
Follow-up US if ≥ 1.0 cm |
| TR5: Highly Suspicious | ≥ 7 | ~35% | FNA if ≥ 1.0 cm
Follow-up US if ≥ 0.5 cm |
Global Context: Comparison with EU-TIRADS and K-TIRADS
While all major risk stratification systems aim to identify thyroid malignancy, they differ fundamentally in their approach and clinical goals.
- Methodology: The TI-RADS calculator employs a point-based system, where specific features are weighted and summed. In contrast, EU-TIRADS (European) and K-TIRADS (Korean) utilize pattern-based systems, where nodules are matched to visual templates or patterns.
- Sensitivity vs. Specificity: The ACR system is optimized for specificity. By setting higher biopsy size thresholds and requiring substantial sonographic evidence to escalate risk, the thyroid nodule risk calculator results in the highest percentage of avoided biopsies among the major guidelines. Conversely, K-TIRADS and EU-TIRADS generally prioritize sensitivity, leading to higher detection rates but a concomitant increase in biopsies of benign nodules.
- The "Blind Spot": Radiologists should be aware that the high specificity of the TI-RADS risk assessment creates a potential "blind spot" for small (1.0-1.5 cm), solid, hyperechoic nodules. These are classified as TR3 and would not undergo biopsy until reaching 2.5 cm under ACR guidelines, whereas other systems might recommend earlier intervention.
Limitations and Pitfalls
Interobserver Variability
While the thyroid ultrasound scoring tool provides a structured lexicon, the subjective nature of ultrasound interpretation introduces variability. While agreement on final biopsy recommendations is generally substantial, concordance for specific features varies:
- Margins: This remains a primary source of discordance. Differentiating between "ill-defined" (0 points) and "lobulated/irregular" (2 points) can be challenging. The lack of strict quantitative criteria for what constitutes a "lobulation" necessitates careful judgment.
- Shape: While "taller-than-wide" is a specific marker, assessing round nodules (where the ratio approaches 1:1) can lead to variability in scoring. Consistent measurement in the transverse plane is required to mitigate this.
Pathology Correlation: PTC vs. FTC
The diagnostic performance of the TI-RADS calculator is strongest for the classical variant of papillary thyroid cancer (PTC), which typically displays high-risk features like microcalcifications and hypoechogenicity. Sensitivity decreases for follicular thyroid carcinoma (FTC) and the follicular variant of PTC. These subtypes frequently present as encapsulated, isoechoic, or hyperechoic nodules which result in lower TR scores (TR3 or TR4), potentially leading to surveillance rather than immediate biopsy despite malignancy.
Special Clinical Scenarios
- Multinodular Goiter: In patients with multinodular goiter, assessing every nodule is impractical. To maintain efficiency, the ACR recommends reporting the four most suspicious nodules, not necessarily the largest. FNA should be limited to a maximum of two nodules with the highest TR scores that meet size criteria.
- Previously Treated Nodules: The thyroid nodule risk calculator is validated for untreated nodules. Prior FNA, thermal ablation, or ethanol ablation can induce hemorrhage, scarring, and architectural distortion. These changes often mimic malignant features (e.g., hypoechogenicity, irregular margins), rendering standard TI-RADS scoring unreliable.
Follow-Up Intervals and Surveillance
For nodules that do not meet the size threshold for biopsy, the ACR TI-RADS committee suggests specific surveillance intervals. These are practice patterns rather than rigid mandates, designed to detect interval growth or morphologic changes.
- TR5: Annual follow-up for up to 5 years.
- TR4: Follow-up at 1, 2, 3, and 5 years.
- TR3: Follow-up at 1, 3, and 5 years.
Cessation of Surveillance: If a nodule demonstrates stability in size and appearance over a 5-year surveillance period, its biological behavior is generally considered benign, and further follow-up may be discontinued.
Frequently Asked Questions
- How strictly should size thresholds for FNA be applied?
The size thresholds (1.5 cm for TR4 and 1.0 cm for TR5) balance cancer detection with the prevention of overdiagnosis. While strict adherence maintains the system’s high specificity, clinical judgment is paramount. Factors such as patient anxiety, comorbidities, or proximity to critical structures (e.g., trachea, recurrent laryngeal nerve) may justify deviation from the standard TI-RADS risk assessment protocols. - How should partially cystic nodules be scored?
Partially cystic nodules are assigned 1 point for composition ("mixed cystic and solid"). However, points for echogenicity, margins, and echogenic foci should be based exclusively on the appearance of the solid component or the nodule periphery. - Do punctate echogenic foci always represent microcalcifications?
Not always. While punctate foci often represent psammomatous calcifications (highly associated with PTC), they can occasionally represent inspissated colloid. The key discriminator is the absence of a large comet-tail artifact. If uncertain, it is safer to score them as punctate foci (3 points) to ensure appropriate risk stratification. - How is taller-than-wide shape defined in practice?
This feature is defined strictly as the anteroposterior diameter exceeding the transverse diameter when measured in the axial (transverse) plane. Measurements taken in the longitudinal/sagittal plane are not used for this determination in the TI-RADS calculator. - Why does ACR TI-RADS use a point-based system instead of patterns?
The point-based system provides a more objective thyroid ultrasound scoring tool that prioritizes specificity. By assigning weights to features based on their statistical correlation with malignancy, the system reduces the subjectivity inherent in "best-fit" pattern recognition models. - When is surveillance preferred over biopsy?
Surveillance is preferred for nodules that meet the TR level criteria but fall below the size threshold for biopsy (e.g., a 0.8 cm TR5 nodule). Additionally, active surveillance is increasingly accepted for small (<1.0 cm), low-risk papillary thyroid microcarcinomas (PTMC) without nodal metastasis or extrathyroidal extension. - How should interval growth be interpreted?
Significant interval growth is defined as a 20% increase in at least two dimensions with a minimum increase of 2 mm, or a 50% increase in volume. If a nodule grows but remains below the FNA threshold for its TR category, the next follow-up is typically scheduled after 1 year. - Can TI-RADS be applied to incidental thyroid nodules?
Yes. ACR TI-RADS was specifically designed to manage the increasing volume of incidental thyroid nodules ("incidentalomas") detected on CT, MRI, or PET scans. Once identified, these nodules should be evaluated with dedicated thyroid ultrasound and scored according to TI-RADS risk assessment criteria. - What is the impact of NIFTP on the guidelines?
The recognition of NIFTP (Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features) as an indolent lesion significantly influenced the ACR guidelines. The higher biopsy thresholds in the thyroid nodule risk calculator aim to avoid over-treating these non-aggressive neoplasms, which previously might have been classified as carcinomas requiring surgery.
Esta calculadora está diseñada para ayudar a radiólogos y especialistas en formación a evaluar el riesgo de los nódulos tiroideos utilizando el Sistema de Reporte y Datos de Imágenes Tiroideas del Colegio Americano de Radiología (ACR TI-RADS). Este sistema de puntuación por ultrasonido de tiroides proporciona un marco estructurado para evaluar nódulos y estimar el riesgo de malignidad, convirtiéndolo en una herramienta valiosa para la toma de decisiones clínicas. Al combinar características ecográficas en una puntuación acumulativa, la calculadora apoya recomendaciones basadas en evidencia para biopsia o vigilancia y agiliza la evaluación del riesgo de nódulos tiroideos en la práctica diaria.
El manejo clínico de los nódulos tiroideos ha evolucionado significativamente con la adopción generalizada del ACR TI-RADS. Diseñado para abordar la alta prevalencia de nódulos tiroideos incidentales detectados hasta en el 68% de los exámenes de ultrasonido de alta resolución y el potencial asociado de sobrediagnóstico, la calculadora TI-RADS proporciona un marco estandarizado y cuantitativo para la estratificación del riesgo de malignidad.
A diferencia de los sistemas europeos (EU-TIRADS) o coreanos (K-TIRADS) que se basan en el reconocimiento de patrones, esta herramienta de puntuación de ultrasonido tiroideo utiliza una metodología basada en puntos. Este enfoque pondera las características ecográficas individuales basándose en su valor predictivo positivo (VPP) para malignidad. Al priorizar una alta especificidad, el calculador de riesgo de nódulo tiroideo tiene como objetivo reducir significativamente el volumen de biopsias por aspiración con aguja fina (PAAF) innecesarias de lesiones benignas o indolentes, manteniendo al mismo tiempo la sensibilidad para enfermedades clínicamente significativas.
Esta guía de referencia detalla la mecánica de puntuación, la interpretación clínica, los matices de los informes y las limitaciones esenciales para radiólogos certificados y residentes que utilizan la calculadora TI-RADS.
Las Cinco Categorías de Características Ecográficas
La evaluación de riesgo TI-RADS deriva una puntuación acumulativa de cinco categorías ecográficas. Los puntos se asignan basándose en la característica más sospechosa de malignidad dentro de cada categoría. Este sistema ponderado asegura que las características de alto riesgo contribuyan desproporcionadamente a la puntuación total generada por la herramienta de puntuación, reflejando con precisión la mayor probabilidad de malignidad.
1. Composición
Esta categoría evalúa la arquitectura interna del nódulo.
- Quístico o casi completamente quístico (0 puntos): Estas lesiones son benignas y no requieren más puntuación.
- Espongiforme (0 puntos): Definido como compuesto por más del 50% de pequeños espacios quísticos, esta apariencia es altamente específica de benignidad.
- Mixto quístico y sólido (1 punto): Esto aplica independientemente de la proporción del componente sólido, siempre que no cumpla con los criterios espongiformes.
- Sólido o casi completamente sólido (2 puntos): Esta característica conlleva una mayor asociación de riesgo. Para fines de puntuación, una estimación visual de >95% sólido es suficiente.
2. Ecogenicidad
La ecogenicidad se evalúa en relación con el parénquima tiroideo circundante y la musculatura anterior del cuello. Para nódulos mixtos, la puntuación se basa exclusivamente en el componente sólido.
- Anecoico (0 puntos): Aplica al fluido quístico.
- Hiperecoico o Isoecoico (1 punto): Ecogenicidad aumentada o similar en relación con el parénquima tiroideo.
- Hipoecoico (2 puntos): Menos ecogénico que el parénquima tiroideo.
- Muy Hipoecoico (3 puntos): Menos ecogénico que los músculos pretiroideos adyacentes (strap muscles). Este es un indicador específico de malignidad y tiene un peso significativo en la calculadora TI-RADS.
3. Forma
La forma se evalúa exclusivamente en el plano transversal (axial).
- Más ancho que alto (0 puntos): El diámetro anteroposterior es menor o igual al diámetro transversal (orientación paralela).
- Más alto que ancho (3 puntos): El diámetro anteroposterior excede el diámetro transversal (orientación no paralela). Esta característica refleja el crecimiento centrífugo contra los planos tisulares y es un fuerte predictor independiente de malignidad.
4. Margen
Esta categoría evalúa la interfaz entre el nódulo y el tejido circundante.
- Liso (0 puntos): Borde ininterrumpido y bien definido.
- Mal definido (0 puntos): El borde se funde imperceptiblemente con el parénquima tiroideo. Es crítico distinguir esto de un margen infiltrativo; los márgenes mal definidos aislados son generalmente benignos.
- Lobulado o Irregular (2 puntos): Bordes espiculados o dentados, o protuberancias hacia el parénquima.
- Extensión Extratiroidea (3 puntos): Invasión franca en tejido blando adyacente o estructuras vasculares. El mero abultamiento de la cápsula no califica como extensión.
5. Focos Ecogénicos
A diferencia de otras categorías donde se selecciona una sola característica, en esta categoría se pueden seleccionar múltiples características y sus puntos son aditivos.
- Ninguno o Artefactos en cola de cometa grandes (0 puntos): Artefactos en forma de V >1 mm de profundidad se asocian típicamente con coloide y benignidad.
- Macrocalcificaciones (1 punto): Calcificaciones gruesas con sombra acústica posterior.
- Calcificaciones Periféricas (en anillo) (2 puntos): Calcificación a lo largo del margen del nódulo. Estas deben ser examinadas cuidadosamente, ya que la sombra completa puede oscurecer componentes malignos centrales.
- Focos Ecogénicos Punteados (3 puntos): Estos corresponden a calcificaciones psamomatosas asociadas con carcinoma papilar de tiroides. Son más pequeños que las macrocalcificaciones y carecen de la cola en forma de V profunda de los artefactos coloides.
Interpretación Clínica: Categorías TR y Manejo con la Calculadora TI-RADS
La suma de puntos determina el nivel TI-RADS (TR). Esta puntuación de evaluación de riesgo TI-RADS se correlaciona con el riesgo de malignidad y dicta los umbrales de manejo basados en el tamaño.
Una característica definitoria del ACR TI-RADS es el uso intencional de umbrales de tamaño más altos para biopsia en comparación con otras pautas internacionales. Este cambio está impulsado en gran medida por la reclasificación de la Neoplasia Folicular de Tiroides No Invasiva con Características Nucleares de tipo Papilar (NIFTP). Reconociendo el NIFTP como una lesión indolente, el ACR estableció estos umbrales para minimizar el sobretratamiento de neoplasias no amenazantes, priorizando la importancia clínica sobre la mera detección.
Tabla: Categorías TR de ACR TI-RADS y recomendaciones de manejo usando la calculadora TI-RADS| Categoría | Puntos | Riesgo de Malignidad | Manejo |
|---|
| TR1: Benigno | 0 | < 0.3% | No requiere PAAF (FNA). |
| TR2: No Sospechoso | 2 | ~1.5% | No requiere PAAF (FNA). |
| TR3: Levemente Sospechoso | 3 | ~4.8% | PAAF si ≥ 2.5 cm
Seguimiento US si ≥ 1.5 cm |
| TR4: Moderadamente Sospechoso | 4-6 | ~9.1% | PAAF si ≥ 1.5 cm
Seguimiento US si ≥ 1.0 cm |
| TR5: Altamente Sospechoso | ≥ 7 | ~35% | PAAF si ≥ 1.0 cm
Seguimiento US si ≥ 0.5 cm |
Contexto Global: Comparación con EU-TIRADS y K-TIRADS
Si bien todos los principales sistemas de estratificación de riesgo tienen como objetivo identificar la malignidad tiroidea, difieren fundamentalmente en su enfoque y objetivos clínicos.
- Metodología: La calculadora TI-RADS emplea un sistema basado en puntos, donde características específicas son ponderadas y sumadas. Por el contrario, EU-TIRADS (europeo) y K-TIRADS (coreano) utilizan sistemas basados en patrones, donde los nódulos se comparan con plantillas visuales o patrones.
- Sensibilidad vs. Especificidad: El sistema ACR está optimizado para la especificidad. Al establecer umbrales de tamaño de biopsia más altos y requerir evidencia ecográfica sustancial para escalar el riesgo, el calculador de riesgo de nódulo tiroideo resulta en el mayor porcentaje de biopsias evitadas entre las principales pautas. Por el contrario, K-TIRADS y EU-TIRADS generalmente priorizan la sensibilidad, lo que lleva a tasas de detección más altas pero un aumento concomitante en biopsias de nódulos benignos.
- El "Punto Ciego": Los radiólogos deben ser conscientes de que la alta especificidad de la evaluación de riesgo TI-RADS crea un "punto ciego" potencial para nódulos pequeños (1.0-1.5 cm), sólidos e hiperecoicos. Estos se clasifican como TR3 y no se someterían a biopsia hasta alcanzar 2.5 cm bajo las pautas de ACR, mientras que otros sistemas podrían recomendar una intervención más temprana.
Limitaciones y Dificultades
Variabilidad Interobservador
Aunque la herramienta de puntuación de ultrasonido tiroideo proporciona un léxico estructurado, la naturaleza subjetiva de la interpretación del ultrasonido introduce variabilidad. Si bien el acuerdo sobre las recomendaciones finales de biopsia es generalmente sustancial, la concordancia para características específicas varía:
- Márgenes: Esta sigue siendo una fuente principal de discordancia. Diferenciar entre "mal definido" (0 puntos) y "lobulado/irregular" (2 puntos) puede ser un desafío. La falta de criterios cuantitativos estrictos para lo que constituye una "lobulación" requiere un juicio cuidadoso.
- Forma: Mientras que "más alto que ancho" es un marcador específico, evaluar nódulos redondos (donde la relación se acerca a 1:1) puede llevar a variabilidad en la puntuación. Se requiere una medición consistente en el plano transversal para mitigar esto.
Correlación Patológica: PTC vs. FTC
El rendimiento diagnóstico de la calculadora TI-RADS es más fuerte para la variante clásica del cáncer papilar de tiroides (PTC), que típicamente muestra características de alto riesgo como microcalcificaciones e hipoecogenicidad. La sensibilidad disminuye para el carcinoma folicular de tiroides (FTC) y la variante folicular del PTC. Estos subtipos frecuentemente se presentan como nódulos encapsulados, isoecoicos o hiperecoicos, lo que resulta en puntuaciones TR más bajas (TR3 o TR4), llevando potencialmente a la vigilancia en lugar de una biopsia inmediata a pesar de la malignidad.
Escenarios Clínicos Especiales
- Bocio Multinodular: En pacientes con bocio multinodular, evaluar cada nódulo es impráctico. Para mantener la eficiencia, el ACR recomienda reportar los cuatro nódulos más sospechosos, no necesariamente los más grandes. La PAAF debe limitarse a un máximo de dos nódulos con las puntuaciones TR más altas que cumplan con los criterios de tamaño.
- Nódulos Previamente Tratados: El calculador de riesgo de nódulo tiroideo está validado para nódulos no tratados. La PAAF previa, la ablación térmica o la ablación con etanol pueden inducir hemorragia, cicatrización y distorsión arquitectónica. Estos cambios a menudo imitan características malignas (por ejemplo, hipoecogenicidad, márgenes irregulares), haciendo que la puntuación estándar de TI-RADS no sea confiable.
Intervalos de Seguimiento y Vigilancia
Para nódulos que no cumplen con el umbral de tamaño para biopsia, el comité ACR TI-RADS sugiere intervalos de vigilancia específicos. Estos son patrones de práctica en lugar de mandatos rígidos, diseñados para detectar crecimiento en el intervalo o cambios morfológicos.
- TR5: Seguimiento anual hasta por 5 años.
- TR4: Seguimiento a 1, 2, 3 y 5 años.
- TR3: Seguimiento a 1, 3 y 5 años.
Cessation of Surveillance: If a nodule demonstrates stability in size and appearance over a 5-year surveillance period, its biological behavior is generally considered benign, and further follow-up may be discontinued.
Preguntas Frecuentes
- ¿Qué tan estrictamente deben aplicarse los umbrales de tamaño para la PAAF?
Los umbrales de tamaño (1.5 cm para TR4 y 1.0 cm para TR5) equilibran la detección de cáncer con la prevención del sobrediagnóstico. Si bien la adherencia estricta mantiene la alta especificidad del sistema, el juicio clínico es primordial. Factores como la ansiedad del paciente, las comorbilidades o la proximidad a estructuras críticas (por ejemplo, tráquea, nervio laríngeo recurrente) pueden justificar la desviación de los protocolos estándar de evaluación de riesgo TI-RADS. - ¿Cómo se deben puntuar los nódulos parcialmente quísticos?
A los nódulos parcialmente quísticos se les asigna 1 punto por composición ("mixto quístico y sólido"). Sin embargo, los puntos por ecogenicidad, márgenes y focos ecogénicos deben basarse exclusivamente en la apariencia del componente sólido o la periferia del nódulo. - ¿Los focos ecogénicos punteados siempre representan microcalcificaciones?
No siempre. Si bien los focos punteados a menudo representan calcificaciones psamomatosas (altamente asociadas con PTC), ocasionalmente pueden representar coloide espesado. El discriminador clave es la ausencia de un gran artefacto en cola de cometa. Si no está seguro, es más seguro puntuarlos como focos punteados (3 puntos) para garantizar una estratificación de riesgo adecuada. - ¿Cómo se define la forma "más alto que ancho" en la práctica?
Esta característica se define estrictamente como el diámetro anteroposterior excediendo el diámetro transversal cuando se mide en el plano axial (transversal). Las medidas tomadas en el plano longitudinal/sagital no se utilizan para esta determinación en la calculadora TI-RADS. - ¿Por qué ACR TI-RADS usa un sistema de puntos en lugar de patrones?
El sistema basado en puntos proporciona una herramienta de puntuación de ultrasonido tiroideo más objetiva que prioriza la especificidad. Al asignar pesos a las características basándose en su correlación estadística con la malignidad, el sistema reduce la subjetividad inherente a los modelos de reconocimiento de patrones de "mejor ajuste". - ¿Cuándo se prefiere la vigilancia sobre la biopsia?
Se prefiere la vigilancia para los nódulos que cumplen con los criterios de nivel TR pero caen por debajo del umbral de tamaño para biopsia (por ejemplo, un nódulo TR5 de 0.8 cm). Además, la vigilancia activa es cada vez más aceptada para microcarcinomas papilares de tiroides (PTMC) pequeños (<1.0 cm) y de bajo riesgo sin metástasis ganglionares o extensión extratiroidea. - ¿Cómo debe interpretarse el crecimiento en el intervalo?
El crecimiento significativo en el intervalo se define como un aumento del 20% en al menos dos dimensiones con un aumento mínimo de 2 mm, o un aumento del 50% en el volumen. Si un nódulo crece pero permanece por debajo del umbral de PAAF para su categoría TR, el siguiente seguimiento generalmente se programa después de 1 año. - ¿Se puede aplicar TI-RADS a nódulos tiroideos incidentales?
Sí. ACR TI-RADS fue diseñado específicamente para manejar el volumen creciente de nódulos tiroideos incidentales ("incidentalomas") detectados en tomografías computarizadas, resonancias magnéticas o escáneres PET. Una vez identificados, estos nódulos deben evaluarse con ultrasonido de tiroides dedicado y puntuarse de acuerdo con los criterios de evaluación de riesgo TI-RADS. - ¿Cuál es el impacto de NIFTP en las pautas?
El reconocimiento de NIFTP (Neoplasia Folicular de Tiroides No Invasiva con Características Nucleares de tipo Papilar) como una lesión indolente influyó significativamente en las pautas de ACR. Los umbrales de biopsia más altos en el calculador de riesgo de nódulo tiroideo tienen como objetivo evitar el tratamiento excesivo de estas neoplasias no agresivas, que anteriormente podrían haberse clasificado como carcinomas que requerían cirugía.






Hi there,
I just used the TI-RADS calculator for a nodule with the following charactristics:
Nodule #1:
– Location: left lobe (mid segment)
– Size: 0.7 cm
– Composition: Solid or almost completely solid
– Echogenicity: Hypoechoic
– Shape: Wider than tall
– Margins: Smooth
– Additional findings: Peripheral/rim calcifications
And it has classed the nodule as TR 4 rather than 5.
Really appreciate the tool 🙂
Hello Orla,
Thanks for your feedback. Based on the characteristics you listed: solid (2), hypoechoic (2), peripheral/rim calcifications (2), smooth margins (0), wider than tall (0), the total comes to 6 points, which corresponds to TR-4. Could you clarify which feature you counted that led to TR-5?
What an incredibly helpful tool! Thank you!